
Solving the Visualization-Access Gap During VL Intubation
During the DL era, the “Difficult Intubation” was defined by a single problem: difficult visualization. Video Laryngoscopy can be thought of as a technical solution designed to solve difficult visualization. VL has successfully solved the vast majority of visualization problems.
As we transition from the DL era into the VL era, a new problem has emerged: difficult tracheal access despite adequate visualization. This challenge is known as the VL Visualization-Access Gap, where a clinician has an adequate view of the vocal cords but cannot successfully pass the endotracheal tube.
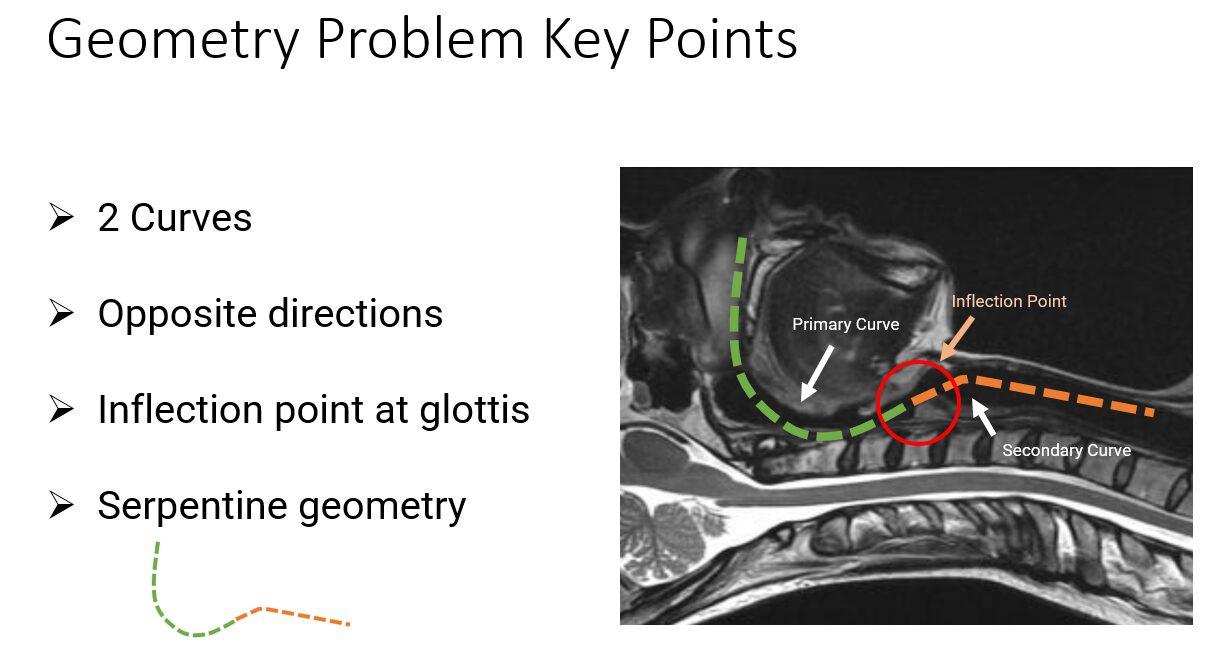
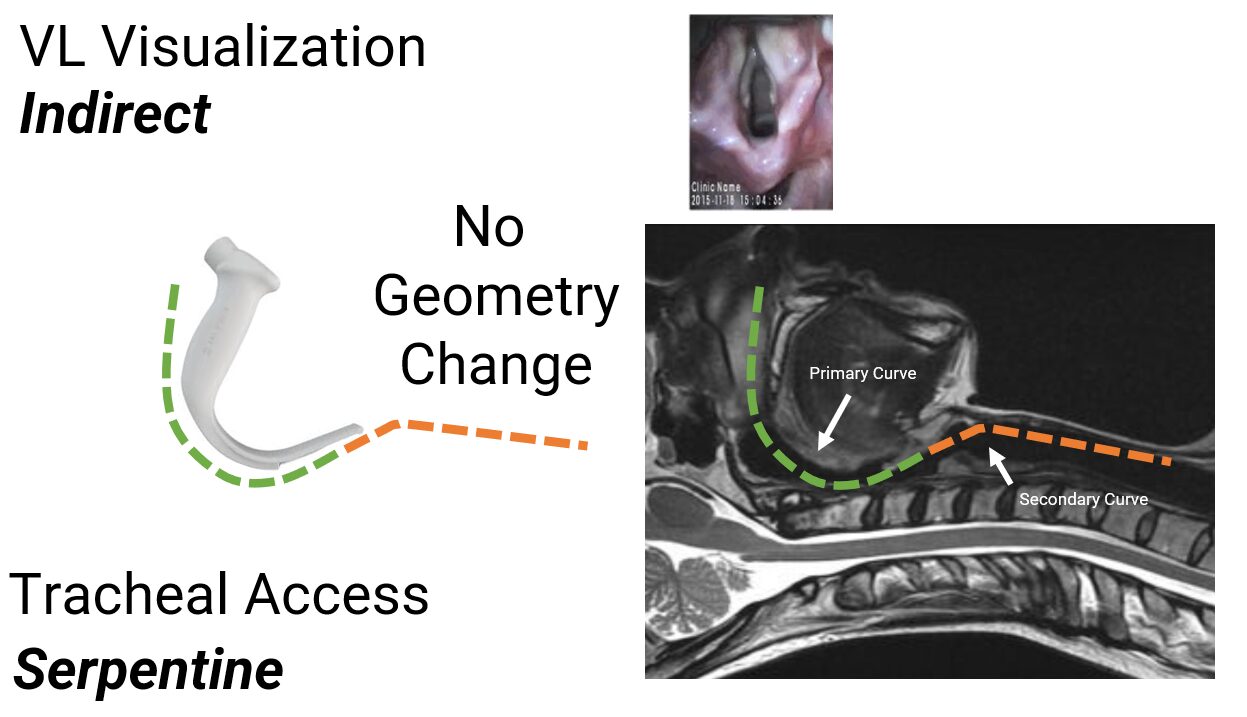
 VL provides a superior view, but it does so without needing to change the natural serpentine geometry of the airway. This means a non-linear, serpentine path to the mid-trachea when VL is used.
VL provides a superior view, but it does so without needing to change the natural serpentine geometry of the airway. This means a non-linear, serpentine path to the mid-trachea when VL is used.
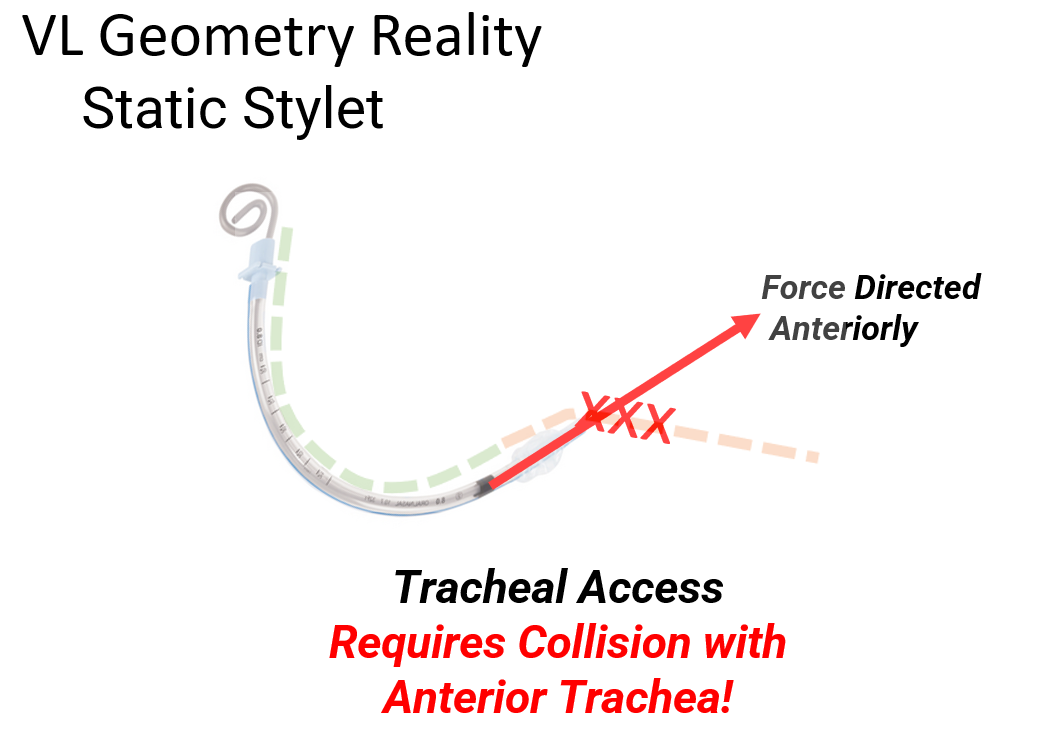
 Traditional stylets and introducers—such as rigid stylets and/or malleable introducers; were engineered for the straight-line geometry of the DL era. Consequently, these tools may be difficult to navigate through the sharper, hyper-angulated serpentine curves associated with modern VL. This geometric mismatch is the root cause of the VL Visualization-Access Gap.
Traditional stylets and introducers—such as rigid stylets and/or malleable introducers; were engineered for the straight-line geometry of the DL era. Consequently, these tools may be difficult to navigate through the sharper, hyper-angulated serpentine curves associated with modern VL. This geometric mismatch is the root cause of the VL Visualization-Access Gap.
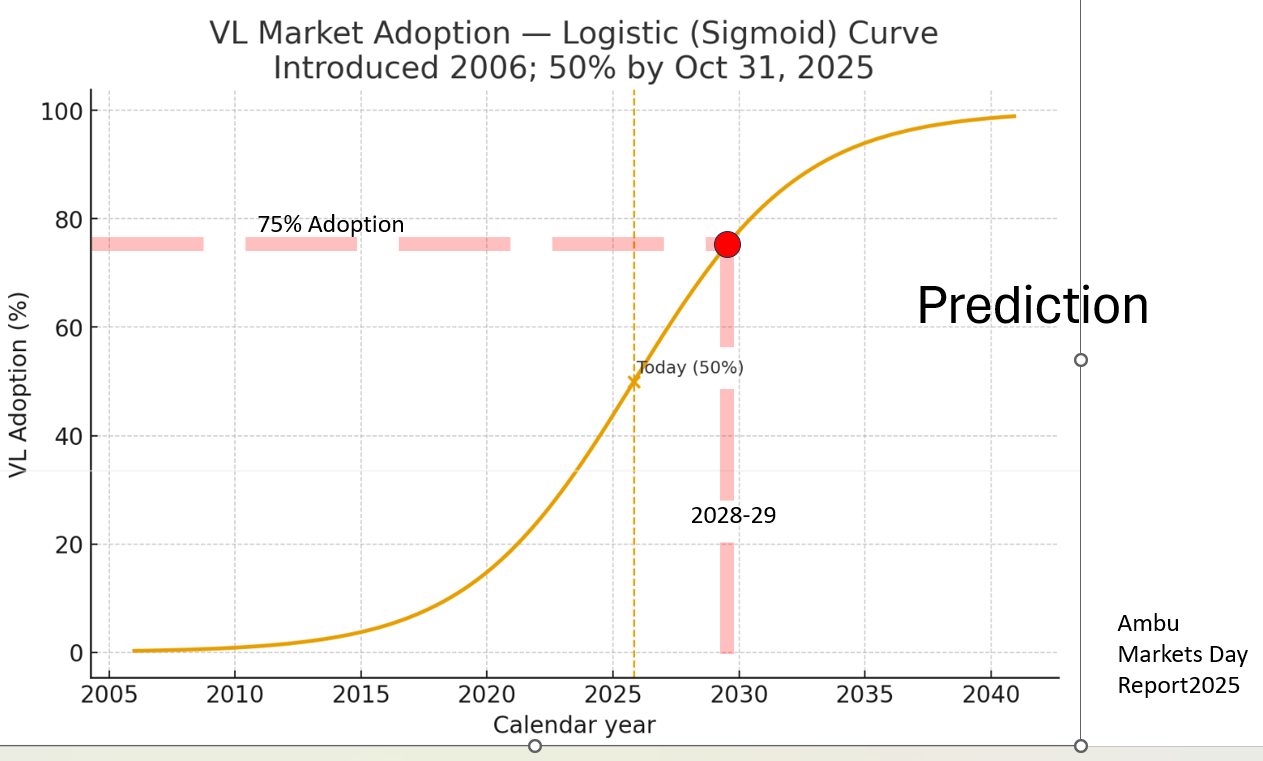
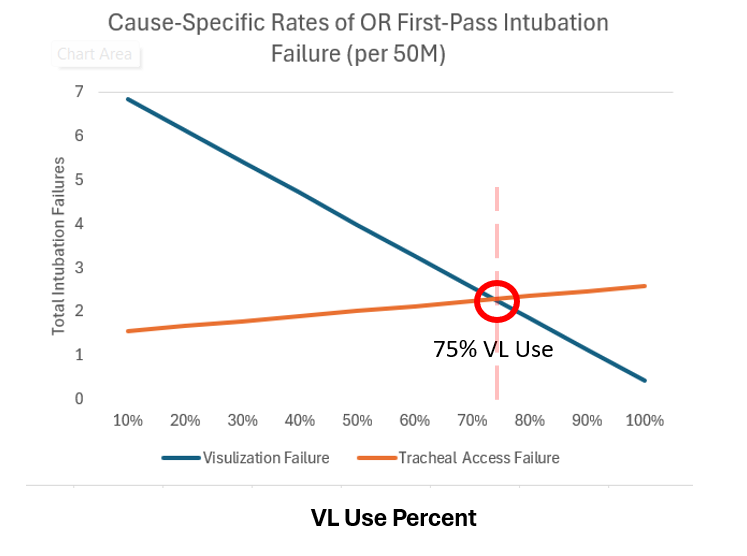 At approximately 75% VL usage, tracheal access failure will eclipse visualization as the primary cause of intubation failure. This eclipse—predicted for late 2028 / early 2029—makes solving the VL Visualization-Access Gap the next great frontier in airway management safety.
At approximately 75% VL usage, tracheal access failure will eclipse visualization as the primary cause of intubation failure. This eclipse—predicted for late 2028 / early 2029—makes solving the VL Visualization-Access Gap the next great frontier in airway management safety.
Understanding the VL Visualization-Access Gap
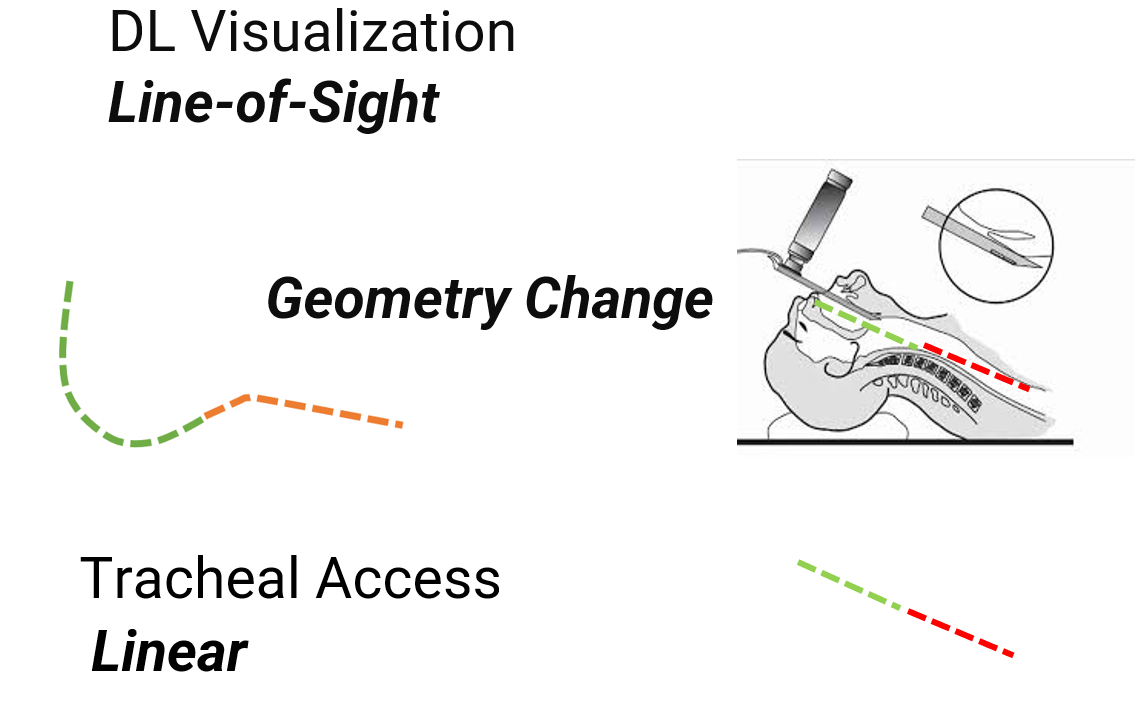
The transition to the VL era has fundamentally changed the geometry of intubation. When DL is used, tracheal access proceeds along a linear pathway (straight bougie is the best friend of DL).
VL provides a superior view, but it does so without needing to change the natural serpentine geometry of the airway. This means a non-linear, serpentine path to the mid-trachea when VL is used.
Traditional stylets and introducers—such as rigid stylets and/or malleable introducers; were engineered for the straight-line geometry of the DL era. Consequently, these tools may be difficult to navigate through the sharper, hyper-angulated serpentine curves associated with modern VL. This geometric mismatch is the root cause of the VL Visualization-Access Gap.
The Magnitude of the VL Visualization-Access Gap
Data presented at the 2025 World Airway Management Meeting (WAMM) reveals a startling trend. Scaled to 25 million annual intubations performed per year in the USA, the math shows that while first-pass failure due to difficult visualization is falling sharply as VL use increases, first-pass failure due to difficult tracheal access is increasing.
At approximately 75% VL usage, tracheal access failure will eclipse visualization as the primary cause of intubation failure. This eclipse—predicted for late 2028 / early 2029—makes solving the VL Visualization-Access Gap the next great frontier in airway management safety.
